Why read a post about mental illness?
- Demographics. Nearly a quarter of the U.S. population will meet criteria for some mental illness this year. Mental illness touches everyone’s life.
- Friendships. Maybe you want to support friends who are suffering. Or you know that increased understanding means a decreased chance of hurting someone you care about.
- Personal Impact. You want to reduce your own chances of experiencing mental illness or cope better with the situation you are in.
- Charity. Perhaps you are someone who wants to “Speak the truth in love.” The more you know, the better you can reach and relate to someone who struggles with mental health.
Whatever your reason, here are five points that might shift your views on mental illness:
1. Mental illnesses are part of the spectrum of common human experience.
I can’t speak for you, but I know I experience anxiety quite often. I remember anxiety over speaking in high school or asking someone on a first date. Now I feel anxiety when others evaluate my work, or when I have to confront someone I care about. I am sure you have worried about some aspect of your life: “Will we have enough to retire?” “Will the principal judge me if my daughter wears mismatched socks and shoes to school?” “Is there something wrong with me if I see the dress as white and gold?” Anxiety and worry are human experiences, but for some they are debilitatingly intense or pervasive.
The criteria for most mental diagnoses are categorical, meaning there is a specific criteria which separates those who fit the diagnosis from those who do not. However, the reality is much less all or none. In reality, the threshold for diagnosis is just one point on a continuum of distress and impairment related to some domain of human experience. Mental illness is our convenient label for those at the most distressed or impaired ends of the continuum of experience.
What does this mean for us? For me, the phrase that springs to mind is “There, but for the grace of God, go I.” I have many of the same qualities as the people I counsel. I have felt sadness, depression, fear, anxiety. I have trouble changing behaviors I find pleasant but which run counter to my values. By the grace of God, the good fortune of genetics, the effort of my parents, and some willingness of my own, those negative experiences have been less intense for me. But that could always change.
I believe that it is actually this commonality of the human experience of emotion that leads some to dismiss anxiety or depressive disorders as a weakness of will. They have experienced emotions like fear and depressed mood, and did not get stuck. The attitude could easily be, “Well if you handled it like I did, you would have the same good outcome.” To me, this ignores many potential differences that place us all at different points on the continuum of mental health. It assumes that everyone has only the liabilities I have, all the advantages I have, and that everyone’s experience of the emotion was the same as mine. Clearly, this is never the case.
2. Mental illnesses manifest with biological differences.
Those at the high end of that continuum of negative experience, those who fit a diagnosis of mental illness, really experience life differently. Our scientific instruments have reached a point where we can point to specific neural activity that is reduced or absent in those with mental health diagnoses. In one sense, we can make a brain-picture of the difference in experience and response to experience as expressed in neural activity.
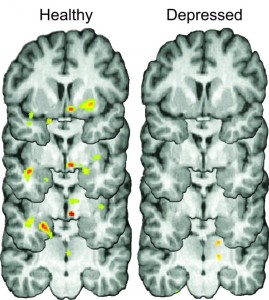
The brains of healthy individuals (left column) released natural opioids during social rejection (colored spots) that may help to reduce negative emotions associated with rejection. In contrast, study participants with depression (right column) did not release nearly as many opioids, which may contribute to a lingering depressed mood following rejection.
Credit: University of Michigan
Here is an illustration by way of an example dealing with the experience of rejection. Researchers examined PET scans of participants while they had simulated experiences of rejection or acceptance by a potential online date. They found marked differences in levels of a common pain and stress-reducing chemical between those with and without diagnoses of depression. Those with depression produced less of the analgesic molecule when rejected. Though they had positive responses to acceptance, they were much more short-lived than the response of non-diagnosed participants.
The takeaway: It is not just as simple as “shaking it off” for many of those with a mental illness. When faced with rejection, those with clinical depression have less neurochemical “pain-killer”. Their natural healing mechanisms are blunted. However it has happened, their brains are changed in ways that make healthy behavior harder. This doesn’t mean that moving on or regaining positive mood is not possible, just that it is a bigger hill to climb.
A metaphor: When I have the flu, I feel much more physically drained by even the simplest tasks. If asked, I am physically capable of getting out of bed and cooking eggs for breakfast. But it would take a huge amount of effort and motivation, I would feel terrible while doing it, and I might burn myself on the pan while cracking eggs cause my hands are shaking that bad. Afterwards, I would probably spend hours in bed recuperating because I don’t have my normal resources for dealing with the physical stress of a normally easy task. The mind and body of someone with clinical depression is affected in ways that are just as physically real as having the flu.
3. We know little about why medications work for many mental health problems.
Drugs targeting mental health work by altering the balance of certain chemicals at the synapses between neurons in the brain. Our knowledge of the brain is rapidly expanding, but the brain is so magnificently complex that we still understand relatively little.
First, we lack a clear roadmap of how, neurologically speaking, many disorders operate. Neuroscientists still debate which models of depression are most accurate. Most models of depression actually were developed after a drug appeared that was effective. The reasoning has often gone like this: “This drug increases serotonin, and many people’s depression improves when they take it. Therefore, depression must be a deficit in serotonin.” Given that state of affairs, it shouldn’t be shocking that many mental health medications were originally developed to treat other medical conditions. During testing they were found to have side effects beneficial to mental health, and were then repurposed and refined for mental health treatment. Without a clear causal pathway, it makes sense that though we know that many medications can be effective, we are less clear about exactly why they are effective.
 Take one common example: antidepressants. They are prescribed to one in ten Americans. Selective Serotonin Reuptake Inhibitors (SSRI’s) are one of the most common anti-depressants, considered relatively safe and beneficial. But we do not actually know why the medication works. For example, we know that the medication prompts higher levels of serotonin at the synapse between neurons within an hour. But it takes 2-4 weeks for the anti-depressant effects to emerge. The mechanism for this intended effect is theorized about, but not known. There is even new evidence that we might have the science completely backwards, and that higher levels of serotonin are worse for depression!
Take one common example: antidepressants. They are prescribed to one in ten Americans. Selective Serotonin Reuptake Inhibitors (SSRI’s) are one of the most common anti-depressants, considered relatively safe and beneficial. But we do not actually know why the medication works. For example, we know that the medication prompts higher levels of serotonin at the synapse between neurons within an hour. But it takes 2-4 weeks for the anti-depressant effects to emerge. The mechanism for this intended effect is theorized about, but not known. There is even new evidence that we might have the science completely backwards, and that higher levels of serotonin are worse for depression!
Many people experience some relief from medication, and some I know say they would not be able to manage without it. My point is not that medication is bad, harmful or should be avoided. It is just that there is far less understanding about psychiatric medication than one would guess from the huge numbers of people using it.
4. Lifestyle changes can provide a huge benefit.
People with mental illness benefit from the same things that are healthy for everyone. Healthy diet, exercise, quality time in relationships, religious and spiritual practices, and serving others all tend to have a positive impact on mental health (pdf) . Oftentimes the magnitude of this impact is as great as that of medication or psychotherapy. Despite this, doctors rarely prescribe diet and exercise changes when people disclose mental health issues.
Turning to religious and spiritual practices can also be a powerful aid in healing. The sacraments are a source of grace and healing. Connecting in religious community enables healthy relatedness. Meditation can be an experience of peace and centeredness. More and more psychological research has documented this, and books on the topic have proliferated. Nevertheless, mental illness often makes religious practice more difficult. Those with a mental illness in church want to receive help through their church, but commonly do not find it offered.
Indeed, the catch is that all these healthy lifestyle changes are often harder to make for someone with a mental illness. I know how many times I have resolved to exercise more, and it is still a challenge for me. I also know how little I feel like doing anything when I am really sad or frustrated. If I mentally put together my natural human tendency to stall and an uncommonly depressed mood, I can have some compassion for just how hard eating right, exercising, or serving others might be.
5. Mental illness has its blessings.
 Yep. Blessings. In this great, brief article about the blessings of mental illness, the author describes how generosity, spirituality, empathy, an accepting spirit, courage and creativity are often gifts of mental illness.
Yep. Blessings. In this great, brief article about the blessings of mental illness, the author describes how generosity, spirituality, empathy, an accepting spirit, courage and creativity are often gifts of mental illness.
Indeed, people often grow from the experience of having a mental illness. When trauma and crisis result in positive changes, this can be labeled “post traumatic growth.” This phenomena has its whole own body of literature, and reflects the ancient wisdom that great good can come from great suffering. Researchers have found that those who endure highly challenging life crises often report:
- An increased appreciation for life in general
- More meaningful interpersonal relationships
- Increased sense of personal strength
- Changed priorities
- A richer existential and spiritual life.
As a New York Times article noted, “Paradoxically, many grow even as they suffer. The way we cope with trauma is far more complex than once thought, and the way it molds us is similarly complex. We bend, we break, we repair and rebuild, and often we grow, changing for the better in ways we never would have if we had not suffered.”
In other posts I have talked about the dangers of avoidance, and how our cultural messages often pave the way towards mental health difficulties. Those who actively battle their illness often emerge with greater awareness of the pitfalls in life and a greater willingness to tolerate suffering. Engaging in self-reflection or psychotherapy can foster a better understanding of self and more humility and compassion for others. Achieving something hard yet meaningful, such as recovering from a mental illness, can foster healthy confidence. At the same time it often requires practicing courage and cultivating hope.
Depression and anxiety disorders are real, and are a great example that God often brings good out of even our negative experiences. After all, our boldest religious symbol is one of intense suffering that yielded amazing grace for all of us. As a Catholic, it makes sense to me that the suffering of mental illness can also yield manifold blessings.
Your turn…
Did you learn something new? Were you reminded of something meaningful? Have something you want to add to this list? Drop a comment below. If you want to subscribe to receive notification of future posts by email, click here. And as always, feel free to share this with anyone who might benefit!
This is the second article concerning awarness of mental illess that I have read on a Catholic blog in 2 weeks. You make great points and I have increased my knowledge of mental illness. Something could be said for the oppostie view though. It is extremely difficult sometimes to deal with someone with mental illness. Especially if that someone is a family member who has had it all her life. For lack of a better way to put this, there are victims of those who have mental illness. The hardest part is when that someone thinks the problem is everyone else who does not see things the way she does. Think of hoarders who make life miserable for those who live with them and get upset when someone tries to do something about it. Or on a macro scale, those who suffer from same sex attraction and are now trying to force their view of reality on everyone else. We are starting to see the cost of not going along with this. I would love to read your thoughts on this side of the coin.
God bless,
Vianney1100
Check out this previous post that talks a little bit about how to support loved ones with a mental illness. It’s more about supporting them, but I think you might find it helpful as well . http://www.psychedcatholic.com/2015/02/gracefully-supporting-friend-mental-illness/
Interesting. I have finally come to terms that for some years now, I have been suffering from depression and it’s gotten worse. I am seeing a counselor, but am getting no sympathy from my siblings. They see me as just pretending. I can assure you, I am depressed and the loneliness and rejection is a big part of it.
KyCatholic, I will pray that you continue to see a counselor and that growth will result from your suffering. My siblings, everyone of us, has issues and each of us suffer from one or more forms of mental illness. I won’t get into the “why” but never the less we all suffer and consequently so do most of the people that love us and care about us. I particularly appreciated the response from Vianney1100 as it hit home with me and illustrated what my family (sisters and myself) has and continues to experience when we interact with each other. The lesson I”ve learned from the article and the few responses so far is that (we) are not the only ones with issues, problems and suffering. It has a name…”Mental Illness” and there is hope and healing if we only seek it. Good Luck to you and God Bless. DOTT in Utah
I’m depressed but forge ahead. I’m angry but I continue to nod politely. I’m sad but I continue to smile. This is my life and many others.
There is a link to a pdf doc at PubMed in section four which I cannot reach. I can see the abstract, but not the document itself. Could a link to the document be provided? It seems it would be a very beneficial document to read.
Try clicking the (pdf) link…if you are at the pub med page,they only have the abstract. I put in the separate link to the pdf on the authors professional website. If you cannot get it to work, google the author name or title from the abstract…
So many falsehoods and so much propaganda, it is difficult to know where to start to critique this harmful article.
I’m at peace with the fact that there are those who peddle the false “sciences” of psychology and psychiatry, and I’ve come to accept the mass drugging of populations. We live in a Fallen World, and evil is a part of that world.
However, I am not at peace with such deception being thrust into the faith community by those who seek to deceive and destroy faith.
Psychology and psychiatry have NOTHING to do with our spiritual existence and our faith journey. Those disciplines attack the very premises of faith, and have no place in the spiritual conversation.
It is time people of faith bar the door and send such peddlers of lies away.
I am sorry that this post offended you. As a faithful Catholic, it is definitely not my intent to degrade Catholic faith. Quite the contrary. If you want to use the contact form to send me an email, I’d be glad to hear more about what you found derogatory to faith.
If it weren’t for Depakote and Attivan my brother would have succeeded in committing suicide. He attempted it three times. This medication has helped him tremendously So don’t knock medication that has helped others who battle mental illness. With mental illness, one’s perception of reality is skewed, including one’s thoughts about faith. If God did not want to help us through various channels, psychiatry would not exist. So don’t knock the means God uses to help those who are suffering from illnesses of the mind.
Excellent !
As a 57 y/o man who has suffered from Depression my entire, though, not knowing until I was 40, I am qualified to comment.
First, the vast majority of people who claim to be mentally fit, cannot identify with mental illness. Second, the way in which mental illness is treat by insurance companies is embarrassing. Benefits usually are at least half of what the they are for physical illness. Third, society continues to shun people with mental illness, which only exacerbates the problem for the sufferer. Fourth, progress is slow in the treatment of mental illness. Medication seems to be the antidote, thus, we see story after story about a mentally ill person doing something outside of societal limits and a family member will invariably mention that the person has not been taking his medication. In doing so, we are asking a person who may not be capable of correctly thinking well of him or her self, to make the decision to properly follow all directions with their medications. I am not so unfortunate, but I know some who are. Fifth, I believe that many of the “demons” Jesus healed people of were in fact, mentally ill. Last, Since my conversion in 2012, the effects of depression have been alleviated a great deal. I still take my medication, and always will need it, and I still suffer from “bouts” of depression, but the Lord has blessed me with an understanding, so that I may be of help to others who suffer likewise.
I hate to sound terribly basic, but what in is the mind?
Gotta define what it is before u can treat it.
Too many models look mostly at the brain.
I suggest that it is the interweaved brain and spirit, and that treating only one is akin to wearing only half of a hat.
Modern therapeutic man believes in chemistry,while jesus’ primary medicine was faith. Not the faith of fundamentalist ‘faith healers, mind you, but faith that sees beyond physical conditions to the deep love that God has for them. Most of us have not even begun to grasp this level of trust He has called us to.
Check out this previous post that talks a little bit about the different aspects of a person, mind, body, spirit, and how reducing mental illness to any one aspect is a disservice: http://www.psychedcatholic.com/2015/01/unhelpful-views-on-mental-illness/
As a mom of a teen with severe depression, I really appreciate this post. I can especially relate the analogy to the flu, having had the flu. It’s one of the hardest conditions to understand, and to bear as a young person, when life is supposed to be full of plans and hope and excitement for the future. My son is just trying to find good reasons to get to tomorrow right now. He is motivated to get better. He is not lazy, and is driving his own recovery. He goes to Confession every week, and prays the Rosary even when he feels like giving up. He is probably the bravest and strongest person I have ever met, because in the full fever of this “flu”, he gets up, gets to class, gets good grades, tries to be a good friend, and child of God. I am in constant wonder. He has said that he would gladly take cancer over this, because when you have cancer, life can stop until you get better. People can see that you are sick and the treatment is for something tangible.
God is good. There are blessings and there is hope, but the mountain is high and the path is always very faint.
Mimi, I am glad you found this affirming! It seems you have also identified a core Catholic value that relates to mental illness: there is value in suffering. I hear that your son is a witness and inspiration to you in his struggle and perseverance and faith. I hope that more people can see his struggle for what it is and lend him support. May God bless you both and grant you healing!
I’m glad you wrote this article. You seemed to focus exclusively on depression and anxiety. I think I know why, and understand, but if an article uses ‘mental illness’ in the title, it seems like it should address a broader scope.
(My brother’s schizophrenia surfaced 10 years ago, and I was eager to read the perspective of a Catholic psychology student.)
Stephanie, the examples I used happened to all be anxiety and depression related. But I think all five points apply to any mental illness. There were a few times I chose to emphasize that anxiety and depressive disorders specifically are real, because they are the most often dismissed. It is often easier for people to recognize illnesses like schizophrenia. I’m curious now as to what the reason was that you had in mind for my focus… Thanks for the comment! If you have any particular questions about schizophrenia (or my perspective on it) just drop me a quick note through our contact form. I hope you and your brother are blessed.
It’s very interesting about whether SSRI’s work or not. I was abused for a long time as a child. There is also mental illness in the family. For 5 years I tried psychotherapy without medication and it worked to a certain degree but I needed more. I got relief but then when through a series of life changes where I became homebound, bedridden 95% of the day and divorced. As pain is a constant companion and other physical conditions have emerged the depression most especially the anxiety has gotten much worse. In the course of these 17 years my prayer life has grown tremendously and I have learned so much more about my Catholic faith through watching EWTN and reading. But still the struggle is huge. It has made me more understanding of others but also aware of the stigma with mental illness that still exists.
I am so grateful I stumbled upon this blog tonight. It is nice to see Catholic psychologists together to discuss different subjects.
After meeting with a counselor over the past year and a half I look back and see how fair I have come in not allowing depression and anxiety to control my life. I have come to have a greater appreciation of my faith, my family and my life. The struggles that I endured (and still do, at times) have made me a stronger person.
I have suffered from bipolar disorder since birth. I am now 68 years old and still suffering. Most people say that their mental illness has gotten them closer to God. I am the opposite. I have just gone through a month-long manic phase during and after which I have lost most of my Catholic/Christian faith. My illness is medication resistant and in fact makes me worse. Now that I am older and don’t drive, I cannot get to church, and no one will take me. I tried having someone come to my house to bring me Communion, but the stress of waiting for them to come was too much for me to bear. I watch EWTN, but instead of it helping my faith, it makes me worse since they are always emphasizing going to Confession and Communion frequently. Since I cannot do that, I feel that I don’t have a chance to make it to Heaven. I am always exhausted because it takes all the strength I have to try and live a normal life as possible. I have accepted the fact that God will not heal me. However, what I find hard to accept is God not helping me at all when I was a young child and afraid I was going to Hell. I feel I envy those who are able to take medication. I don’t know how I have survived this far, but now that I’m getting close to death, I am afraid every day of going to Hell since I cannot get to church.
Thanks for the fine article on faith and mental illness. As one with the latter, faith helps.